Commentary by a toe doctor

YOSHIRO YUASA
Keiro Yuasa
Physical Therapist, Doctor of Toes, Director of Toe Research Institute, President of the Japanese Society of Functional Foot and Toe Therapy, and developer of Halmek shoes. Former director, vice president, and medical director of General Hospital. His specialties are exercise physiology and anatomy. He is also a foot and shoe specialist and a leading expert in postural occlusion therapy. He has cured various orthopedic diseases (over 70,000 people) with toe therapy alone.
Long before Chris McDougal and "Born to Run," there was a Dr. Phil Hoffman who was ahead of his time: more than 100 years ago, in 1905, Dr.Journal of the American Academy of Orthopaedic Surgeonspublished a study entitled "Conclusions Drawn from a Comparative Study of Barefoot and Shoed Feet," which has been largely ignored for more than a century. During the discussion, Dr. Henry Ring Taylor praised Dr. Hoffman's interesting research and recommended that the results of this study be "widely disseminated and made known to the general public." So here is the paper that Dr. Hoffman, the pioneer of barefoot running and father of the minimalist shoe, published 100 years later. It is a bit long, so I hope only those interested will read it.
Conclusions from a comparative study of barefoot and shoe-wearing people's feet
long vowel mark (usually only used in katakana)Phil Hoffman, M.D., St. Louis.
A study of the feet of 186 pairs of individuals who had never worn shoes was conducted by a group of Central African and Pygmy tribes.
subject (of taxation, etc.)
- General observations comparing the feet of barefoot competitors with those of competitors wearing shoes. This includes the shape and function of the foot, the range of voluntary and passive movement, and the overall length and relative length of its component parts.
- The height and shape of the longitudinal arch and its effect on the usefulness of the foot.
- Whether there is a relationship or coincidence between arch height and gait.
- Specimen collection.
method
Measurements of height, foot length, and foot component parts were taken, as well as records regarding gait. To collect data on foot shape and mobility, footprints were left on smoked paper and plaster casts were made to assess foot expansion and arch sink. In addition, cameras were used to record toe movements during tree climbing and grasping, and foot postures during standing and walking.
Conclusion.
From these observations and the study of the data, we were able to draw the following conclusions The relative length of the foot to height and the ratio of phalanges to foot length were found to be approximately the same whether barefoot or with shoes on. This trend continues from toddler to adult.
We found that up until the time they begin wearing shoes (usually around one year of age), there is no significant change in the shape or movement of the foot, whether barefoot or with shoes on, but with shoes on, the front of the foot becomes narrower and the range of motion of the joints is restricted.
Modern footwear is designed according to people's sense of aesthetics and manufacturers' preferences, rather than according to the general shape of the foot. Although society tends to view small feet as beautiful and admire the skills of shoemakers, it has become clear that the shape is actually dictated more by manufacturer convenience and fads than by the natural shape of the foot. This suggests that the choice of footwear influenced by appearance and fashion rather than proper support and comfort for the foot should be considered problematic.
It's the same today, with manufacturers' convenience and fashions dictating the form.
Negrito leg
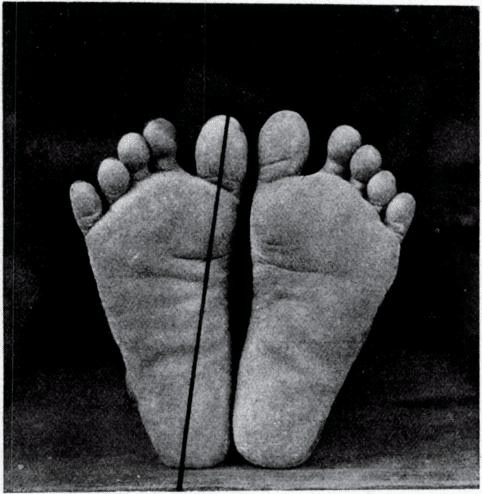
Figure 1.-Base view of a Negrito foot. It shows that the toes are straight and far apart, that there are transverse folds in the skin of the sole, that the toes are the widest part of the foot, and that the long axis of the thumb extends backward and touches the center of the heel.
A symptom that seems to be universal in adults wearing shoes is the overlapping or hiding of the toes with the adjacent toes. This symptom is especially common when the thumb is hidden under an adjacent toe. Figure 6 compares the condition of such a foot with the shoes worn on that foot. Comparing the pictures, we can see that the toes are compressed, the front of the foot is narrower, and the line extending backward from the long axis of the thumb falls inward at the heel. This foot shape is especially common among women and is the cause of foot deformities caused by shoes. We can also see that the shoes are not properly shaped and that the shoes are too small because the feet are already deformed. These foot deformities may not only be caused by the shoes, but also by years of overuse. These illustrations are interesting examples of the effects of common shoe types on the feet.
YOSHIRO SOCKS are derived from the "original foot shape" shown in this photo
Bagobo's.leg
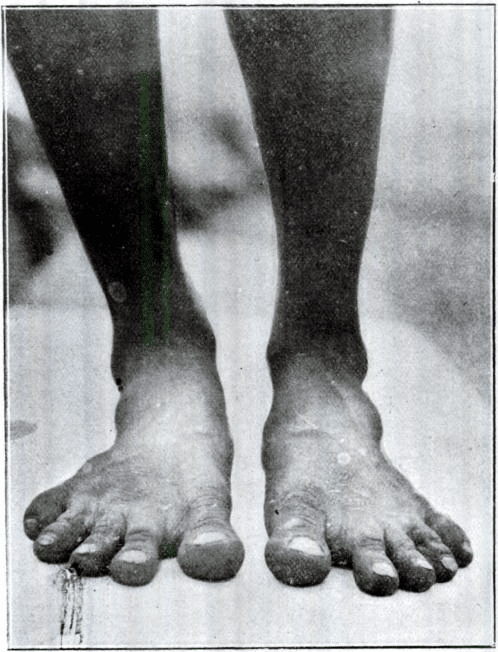
Figure 2.-Dorsal view of the weight-bearing foot of a bagobo. It shows the separation of the toes, the adduction of the thumb, and the minute folds of the skin.

Figure 3.-Hermes' foot in Praxiteles. It can be seen that the toes are straight and apart.
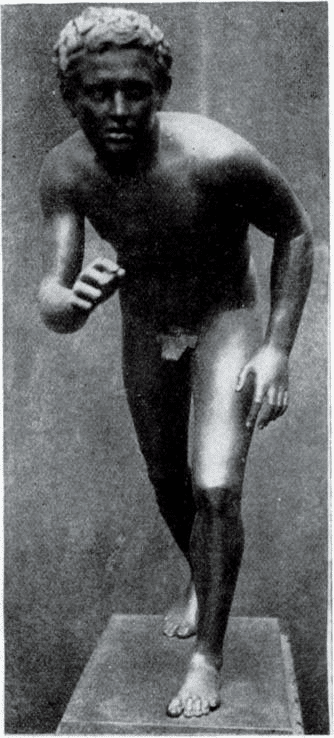
Figure 4.-Ancient bronze from Herculaneum, showing foot and thumb adduction.
Chingalese.leg
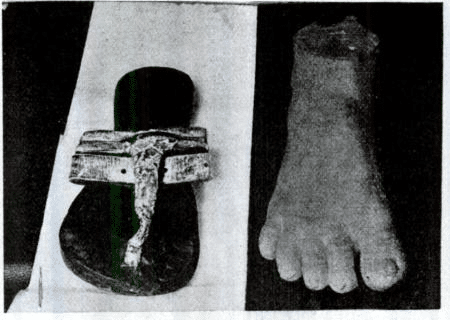
Figure 5.-Photograph of a Chingalese weight-bearing foot mold and sandals. The foot shape is similar to that of the modern barefoot race and ancient sandal-wearing peoples.
Foot affected by footwear
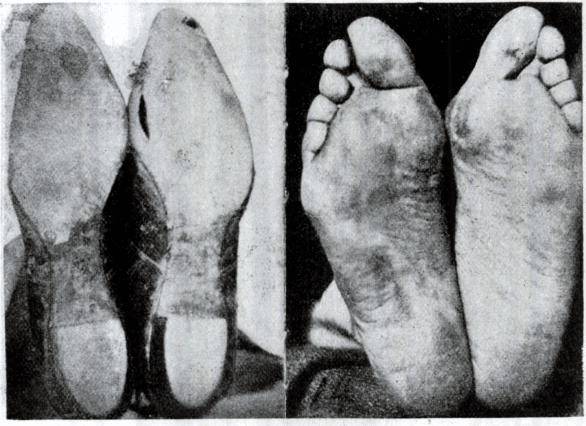
Figure 6.-Common types of footwear and their inevitable effects. The shape of the foot matches the shape of the shoe.
When examining an infant's feet, it is important to do so without shoes on. Check to see that the toes are clearly separated and that adjacent toes are not crushed together. Also check that the big toe and little toe are in line with the metatarsals and that the medial edges of the foot are aligned. In a normal foot, the long axis of the big toe, when extended backward, should be located around the center of the heel. Evidence of this is evident in the shape of the barefoot adult foot, which shows that proper foot shape is maintained throughout life. (Figure 1 and Figure 11. B)
Today, we no longer wear shoes that can push in so hard, but another problem has led to toe deformities.
Feet of a person wearing high heeled shoes

Figure 7.-Hyperextension and interphalangeal flexion of the anterior metatarsal phalanges.
You have completely "floating" and "flexing" fingers.
Wearing high heels, especially stooped high heels, places a very heavy burden on the feet because they must balance on the front part of the foot. This habit may cause many middle-aged women to have difficulty bending their knees and dorsiflexing their feet as their calf muscles shorten.
Wearing shoes can cause the toes to become hyperextended for long periods of time. Wearing shoes with a high heel or crowded toes can cause deformities of the foot and toe joints. (Figure 7)
Among shoe-wearing adults, a foot without pressure deformity should be extremely rare. I have never seen such feet, except in cases where it is impossible to wear normal shoes, i.e., when a person has a congenital clubfoot and wears shoes that do not compress the toes. As an example of how familiar civilized society is with certain foot deformities and how unaware the average person is of his or her own foot deformity, it was displayed as an advertisement in a show window, printed as "one of the best built athletes in the world," even though the foot deformity is obvious, This is sometimes accepted as a common situation.
China's gargantuan feet
Young people's feet are highly plastic and can be deformed into almost any shape by prolonged pressure. Consider, in particular, the deformations of the feet performed by high caste women in China. Through a system of bandages, starting at the age of five or six, these women would bend the front half of their feet to the extreme, adjusting their toes and heels to fit into small shoes. As a result, their feet were reduced to the size of a teacup.
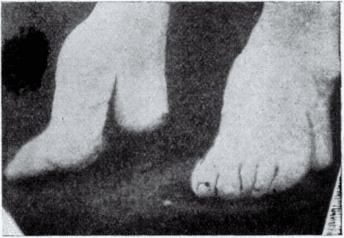
Figure 8.-A high caste Chinese woman's foot with typical deformity caused by bandages.
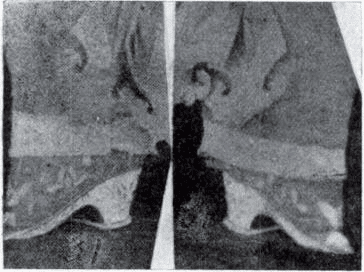
Figure 9.-Shoes worn on the feet depicted in Figure 8.
It is said that this made it difficult for these women to stand still on a flat floor and they had to constantly walk back and forth. Yet why do we still laugh at this practice of Chinese women? In other countries, too, we see the practice of deforming feet by wearing shoes that are half as small as they are wide. Wearing shoes so small that both toes and heels disappear, as well as unstable heels, can deform and hurt the feet.
It is not only Chinese women that such practices should be considered problematic, but also in other countries. The difference may not be in the type of custom, but in the degree. Considering that people tend to follow what has been ingrained in them from childhood, and that the effects of such practices can be harmful to their own health, we need to be objective about the practices of various cultures.
The last time the gargantuan footwear was used was in 1957.
Experiment in Bagobo Village
Interesting research has been conducted in the village of Bagobo regarding the effects of prolonged shoe wear on young feet. On September 22, I took molds and tracings of the feet of some residents, including a 12-year-old boy and an 8-year-old girl. Then on November 16, I again took foot molds and tracings of all families in the village, including these children. The resulting comparisons showed a clear difference between the old and new tracings. In the new tracings, the front of the foot was narrower and the orientation of the thumb had changed (Figure 10).
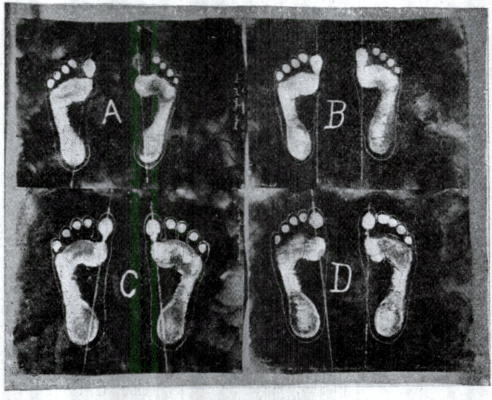
Figure 10.-Footprints and footprints of children in Bagobo. The effects of wearing shoes for several weeks can be seen; A and C are before wearing shoes, B and D are after. Note the narrowing of the front of the foot and the change in direction of the long axis of the thumb.
The cause of this change was found to be that the climate turned colder in late October and the Bagobos began to wear shoes instead of their traditional clothes. The shoes they wore were conventional American-made shoe molds, which did not fit their feet at all, especially a 12-year-old boy with severe foot deformities. He had originally worn the shoes in his hometown, which caused even more advanced deformities. Figure 11 shows the results of comparing the plaster cast of his feet with those of an adult male who had never worn shoes.
Many Bagobos experienced little discomfort when wearing the shoes for the first timeIt was noteworthy that the The shoes were about half the width of a normal foot, and the pressure on the foot did not seem to be very uncomfortable. An experiment was then conducted to investigate the extent to which the feet could be compressed without pain. In the case of the adult male, the range of pressure that could be applied without pain was greater, but not as great as in the case of bare feet. We found that prolonged compression, painful or not, could cause irreparable damage.
You don't feel the pressure of the shoes at the beginning of wearing them, but over time, your feet are most likely deformed before you know it. You don't know it yourself.
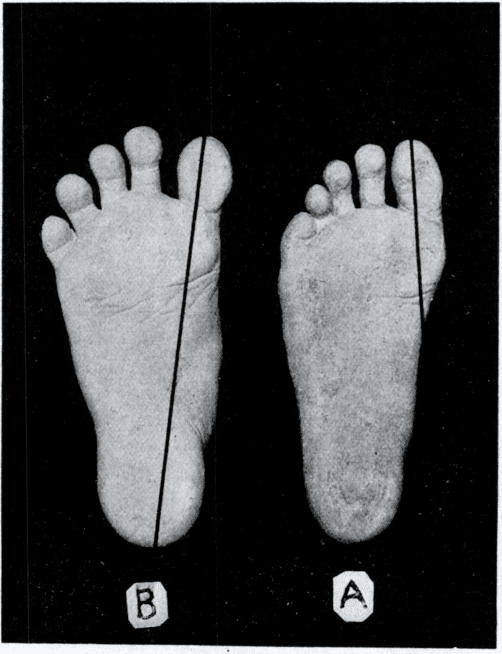
Figure 11.-A. Comparison of a photograph of a plaster cast of the foot of a Bagobo boy who wore shoes for several months and B. A photograph of a Bagobo adult who has never worn shoes.
The figure below shows the foot and shoe shapes of shoe wearers. The solid line represents the shape of the foot and the dotted line represents the shape of each shoe. These are general shapes and reflect the pressures that millions of people experience on a daily basis. Over time, the foot becomes accustomed to the pressure and becomes less aware of it.
You get used to the pressure on your feet; at the end of the day, you can relieve foot fatigue with the "Hironoba Exercise.
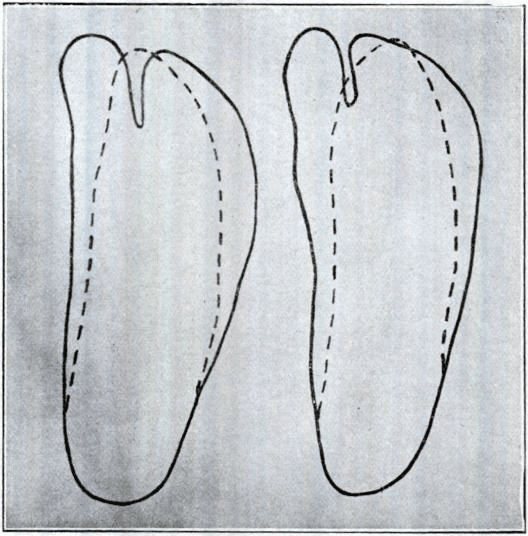
Figure 12.-The extent of painless pressure on the feet in barefoot people. Bontoc Igorote and Moro. The solid line shows the normal foot contour and the dotted line shows the painless contour of the same foot under manual pressure. Compare with Figure 13.
Shoes worn on a daily basis can negatively affect foot function by depriving the foot of the free movement of many small joints. Shoes can restrict foot movement and inhibit the free movement of the toes. Typically, the toes can hyperextend to near right angles and flex beyond 1 degree. The range of adduction of the medial tarsal joint is between 30 and 40 degrees. The infant's foot reveals that the toes can spontaneously separate and spread laterally. In contrast, such free movement is rarely seen in the feet of adults wearing shoes. Depending on the type of shoe, the ability to spread the toes laterally may be lost. Some tribal adults who walk barefoot may still retain some foot function, but this function may be limited by wearing shoes.
Even today, shoes still limit the function of the foot, and YOSHIRO SHOES is designed to improve the function of the foot, and will be further updated in the future.
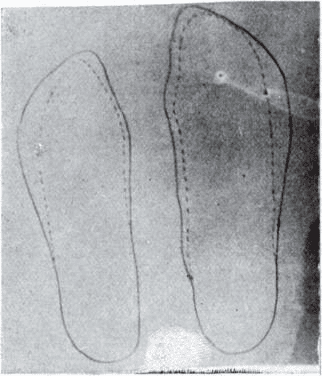
Figure 13.-Range of painless pressure on the shoe-worn foot. Compare with Figure 12.
Since most adults wear shoes, the toes typically do not perform much function other than lengthening the length of the foot. In barefoot people, on the other hand, toes perform a variety of functions, including climbing and grasping trees (Figures 15, 16, 17, 18). This is attributed to the difference between the toes developing through daily use and the toes being inhibited in people who wear shoes. Toes are not congenitally different in structure, but their function is altered by daily use and development. Toe function may develop similarly in people who wear shoes.
Each toe has its own role; simply put, they are like sensors for balance.
For example, a young man who was born without hands can perform many functions normally used by his hands by thoroughly training his toes. Not only can they use knives and forks, combs and brushes, pens and ink, but they can also wash themselves, dress themselves, play the piano, and so on. While this is an unusual case, it is a good example of the flexibility and wide range of uses for the feet.
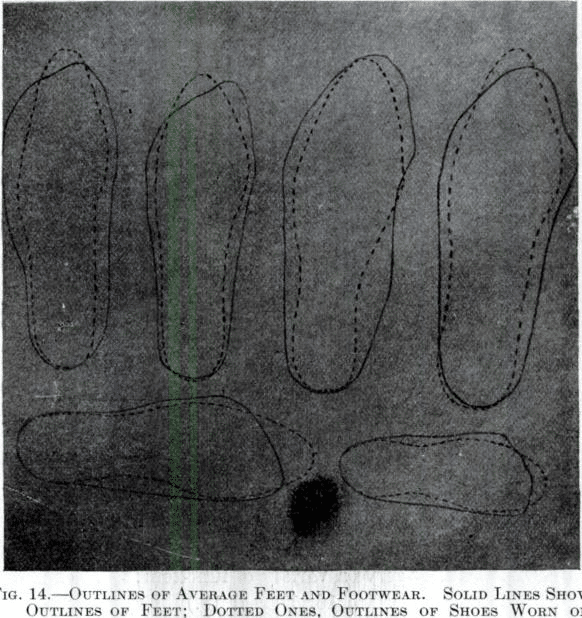
Figure 14.-Average foot and footwear contours. The solid line shows the foot contour and the dotted line shows the contour of the shoes worn on these feet.
Ancient sandals did not compress the toes or impede their independent movement. The result of this freedom is evident in classical sculpture, which depicts the powerful toe movements in the figures of many athletes. A particularly good example is the right foot of the famous discus thrower attributed to Mullon (Figure 19). The athlete's toes firmly grip the ground and help to keep the athlete stable, with all muscles tensed and in optimal position as he moves his arms forward.
It is also important to note that modern sandals and ancient sandals are made differently. If you wear sandals thinking that they are good for your health, they will deform your toes.
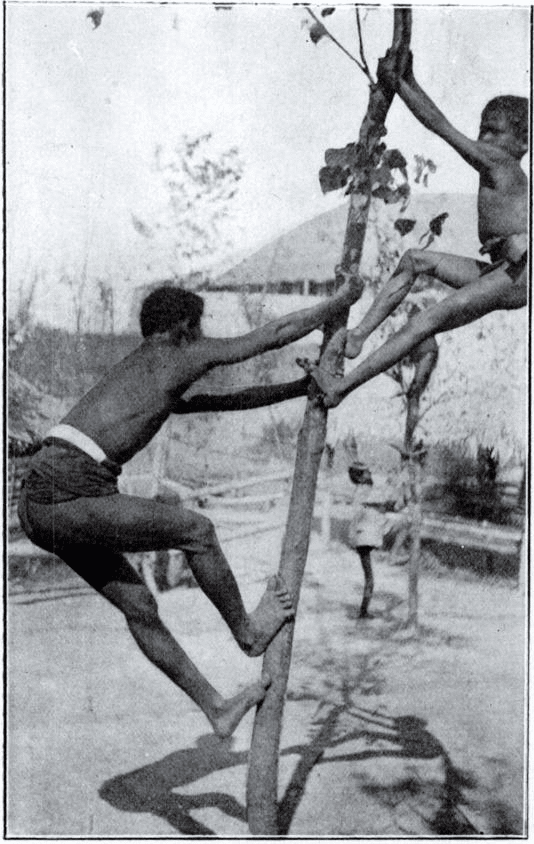
Figure 15.-Negrito tribe, using toes for climbing.
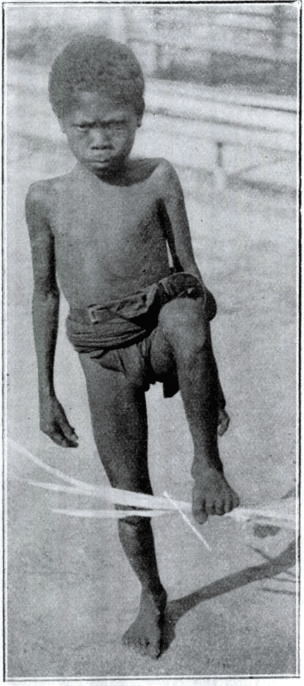
Figure 16.-Negrito boy grasping an object with his toes.
In modern times, we wear shoes to climb trees, so we use the non-slip function of the soles of our shoes, so the function of our feet degenerates.
Skin of the foot
My attention was especially drawn to the skin covering the pristine feet. It is remarkably similar to the skin of the hands. The skin of the sole is thick and tough, but very flexible, without the callus-like patches of friction often seen in shoe wearers. There are deep transverse folds corresponding to the flexure lines of the joints, similar to those universally present on the palms of the hands (Figure 1 and Figure 11. B). The dorsal skin has many fine but distinct folds similar to those found on the back of the hand (Figure 2). The depth and distinctness of these folds in barefoot individuals may be due to the almost constant movement of the phalangeal and tarsal joints, which results in intermittent folds of skin.
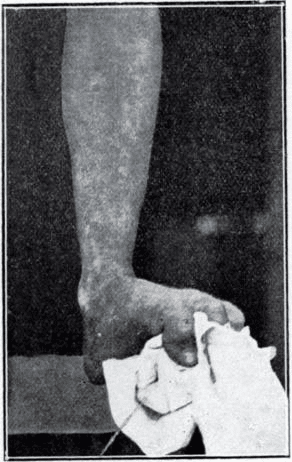
Figure 17.-Grasping function of the primitive foot.
foot arch
Observations of the longitudinal arches of the foot have shown that their height and shape are not decisive factors in estimating the usefulness of the foot, and that there is no single normal type, but rather high, moderate, and low arches in the normal foot. While it is true that moderately high arches are predominant, we cannot assert that even the presence of very low arches is a sign of weakness. It has also been observed in the cases of primitive Filipinos and Africans that low arches are associated with strong, flexible feet. Low arches are a fact and not merely an effect of the fat located underneath. It is clear that a surgeon's impression record of the longitudinal groove of the foot is worthless in diagnosing the commonly recognized flat foot. Symptoms of flatfoot are due to debilitating arch weakness and not solely to low arches. However, low arches may be due to a change from an originally high arch, unless the condition is affected by the relationship of the tarsal bones, ligaments, or muscles. Such changes, however, are considered rare. Similarly, symptoms associated with high or abnormally high arches are often observed. Low arches may also be seen in the symptomless foot.

Figure 18.-Bagobo woman. She uses her toes as a third hand to hold the thread taul.
Examined.Of the 186 pairs of caveman feet, not a single foot was found with symptoms of weakness characteristic and common to shoe-wearing adult feet.It is very significant that the They are weakened by the limitations that shoes place on their function. Through our interpreters, we carefully investigated this point, especially when we found feet with abnormally low arches.
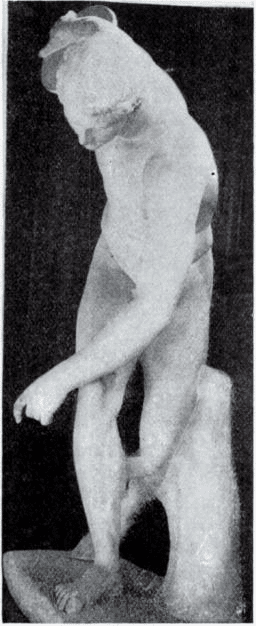
Figure 19.-Muron discus thrower, showing powerful toe movement.
Figure 20 illustrates several types of arches found on the normal foot. These records usually indicate the degree to which the sole is in contact with the ground and do not directly indicate the height of the longitudinal arches. However, they are usually associated with arch height, so when we use these records to refer to height, we do so in that sense.
Comparison of the smoked impression and the plaster mold showed that the areas of the foot that flattened when weight was applied matched. This indicates that weight compression can accurately identify the area where weight was applied. The plaster molds also showed that the relationship between the inward spread of the sole impression and the lower arch is almost constant. In other words, the more the impression extends inward, the lower the arch height.
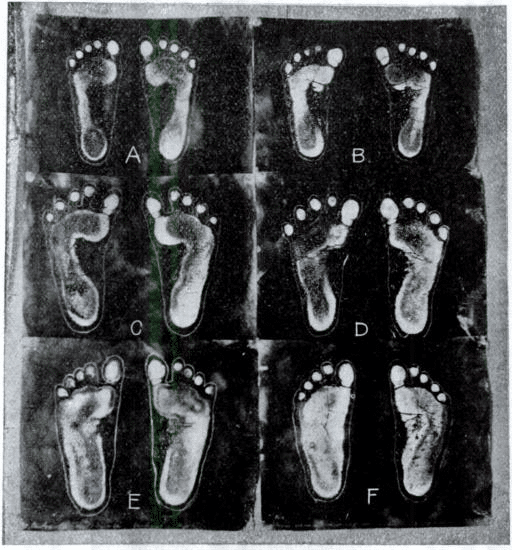
Figure 20.-Some of the types of arches found in the normal foot.
Type of arch in the foot of a person who has never worn shoes (data)
The following table shows the frequency with which the various types appeared in the 186 barefoot subjects examined. Of course, the most similar types include many intermediate levels. (Decimal points in percentages are omitted)
| Arch type | the number of people | % |
|---|---|---|
| A | 4 | 8 |
| B | 6 | 13 |
| c | 7 | 15 |
| D | 7 | 15 |
| E | 9 | 19 |
| f | 13 | 28 |
| 46 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| A | 2 | 7 |
| B | 6 | 22 |
| c | 5 | 18 |
| D | 4 | 14 |
| E | 5 | 18 |
| f | 5 | 18 |
| 27 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| c | 1 | 33 |
| E | 2 | 66 |
| 3 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| A | 6 | 8 |
| B | 2 | 2 |
| c | 8 | 11 |
| D | 24 | 34 |
| E | 18 | 25 |
| f | 12 | 17 |
| 70 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| A | 3 | 9 |
| B | 4 | 12 |
| c | 5 | 15 |
| D | 6 | 18 |
| E | 6 | 18 |
| f | 9 | 27 |
| 33 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| A | 15 | 8 |
| B | 18 | 10 |
| c | 23 | 14 |
| D | 41 | 22 |
| E | 40 | 22 |
| f | 39 | 21 |
| 179 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| A | 2 | 28 |
| B | 1 | 14 |
| D | 2 | 28 |
| E | 1 | 14 |
| f | 1 | 14 |
| 7 | 100 |
| Arch type | the number of people | % |
|---|---|---|
| A | 17 | 9 |
| B | 19 | 10 |
| c | 26 | 14 |
| D | 43 | 23 |
| E | 41 | 22 |
| f | 40 | 21 |
| 186 | 100 |
Types of arches for black South Africans
In addition to the 186 barefoot people on whom these statistics were based, I have 15 black South Africans, i.e.The Matabele, Zambezi, and Hottentot tribes were surveyed. They all remained barefoot until early adulthood and have only been wearing shoes for the last five to six years. Table 9, which summarizes their footprint records, may be of interest in showing the frequency of different types of arches in this group.
| Arch type | the number of people | % |
|---|---|---|
| A | 6 | 13 |
| B | 7 | 15 |
| c | 8 | 17 |
| D | 7 | 15 |
| E | 11 | 24 |
| f | 6 | 13 |
| 45 | 100 |
Types of arches for whites and blacks wearing shoes
Table 10 shows that there is as much variation in the height and shape of the longitudinal arches in Caucasian shoe wearers as in barefoot people. This table is based on examination of 200 pairs of normal or at least symptom-free feet.
| Arch type | the number of people | % |
|---|---|---|
| A | 27 | 13 |
| B | 20 | 10 |
| c | 27 | 13 |
| D | 53 | 26 |
| E | 40 | 20 |
| f | 33 | 16 |
| 200 | 100 |
That the same is true for blacks wearing American shoes is shown in Table 11, based on an examination of 100 pairs of asymptomatic feet.
| Arch type | the number of people | % |
|---|---|---|
| A | 18 | 18 |
| B | 13 | 13 |
| c | 19 | 19 |
| D | 21 | 21 |
| E | 16 | 16 |
| f | 13 | 13 |
| 100 | 100 |
Type of arch of the Ainu people
Table 12 shows the changes in the five Ainu who wore sandals.
| Arch type | the number of people | % |
|---|---|---|
| B | 1 | 20 |
| c | 1 | 20 |
| D | 1 | 20 |
| E | 2 | 40 |
| 5 | 100 |
Type of arch of Caucasian wearing shoes
It is correct to point out that structural weakness of the longitudinal arch can sometimes cause arch sinking, which results in a larger area of the foot in contact with the ground. However, my examination of the 560 footprints I treated showed that although almost all of the feet showed typical symptoms of longitudinal arch weakness, almost all were receiving arch support, and arch sinking was not frequent or pronounced. Actual,Average foot type characteristics used for diagnostic purposes are almost identical to the average characteristics of a healthy foot without symptomsThe results of the study showed that the Details are summarized in Table 13.
| Arch type | the number of people | % |
|---|---|---|
| A | 64 | 11 |
| B | 72 | 12 |
| c | 76 | 13 |
| D | 92 | 16 |
| E | 108 | 19 |
| f | 148 | 26 |
| 560 | 100 |
Summary of data
Table 14 shows a comparison of the frequency with which the various types of arches shown in Figure 20 occur in Filipino Malays (barefoot), Central African blacks (barefoot), South African blacks (barefoot for 6 years), American blacks (shoe wearers), Caucasians (shoe wearers), Ainu, Caucasians, people from northern Japan (sandal wearers) (all with symptomless feet), and Caucasians (shoe wearers) undergoing treatment for symptoms of vertical arch weakness. The following table shows a comparison of the frequency of occurrence in Caucasians (shoe wearers) undergoing treatment for symptoms of longitudinal arch weakness.
| Arch type | Philippines | Blacks in Central Africa | Black South Africans | Blacks in America | Caucasians, shoe wearers | Ainu, Caucasian, Northern Japan | Caucasian person |
|---|---|---|---|---|---|---|---|
| Type A | 8% | 28% | 13% | 18% | 13% | — | 11% |
| Type B | 10% | 14% | 15% | 13% | 10% | 20% | 12% |
| Type C | 14% | — | 17% | 19% | 13% | 20% | 12% |
| Type D | 22% | 28% | 15% | 21% | 26% | 20% | 16% |
| Type E | 22% | 14% | 24% | 16% | 20% | 40% | 19% |
| Type F | 21% | 11% | 13% | 13% | 16% | — | 26% |
| 100% | 100% | 100% | 100% | 100% | 100% | 100% |
Of the 536 individuals of different races with symptomless feet from the analysis in Table 14,Americans and primitive blacks had a lower percentage of low arches and a greater percentage of high arches than whitesIt can be seen that This contradicts the generally accepted view. We find that the Filipino Malays had somewhat larger percentages of low arches than either the blacks or the whites. Another point shown in this table is that the feet of 560 symptomatic whites with weakened arches did not have as large a percentage of low arches as those of whites without symptoms. The history accompanying these 560 impression records indicates that symptomatic long-term or severely symptomatic feet did not have more low arch type feet than those with mild or short-term symptoms.
With modern plantar pressure measuring equipment, we could have done more analysis.
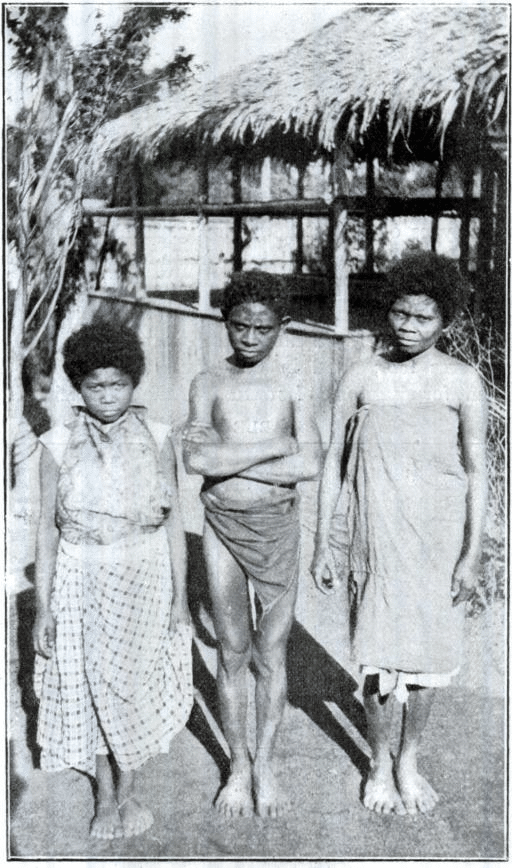
Figure 21.-Photograph of Negrito showing habitual foot posture while standing.

Figure 22.-Photograph showing the habitual foot posture of the Negritos when walking.
If these statistics are fair indicators that apply to all feet, they justify the conclusion that weakness of the longitudinal arch rarely leads to arch-sagging and that flatfoot as a pathological entity rarely exists.
Arch height has nothing to do with how you walk.Appears to be. In shoe wearers, the condition commonly referred to as flat feet often causes the foot to turn outward more than normal when standing or walking. This outward contraction is not due to low arches, but to weakness or stiffness in the joints of the feet and the muscles that control those joints.Walking with your toes pointing forward means using your feet as leverage to lift and propel your bodyThis implies muscle tension and joint movement. To avoid this action, the weakened leg is externally warped. The more the eversion progresses, the less use is made of the leverage function, which eventually degenerates into a mere pedestal for weight bearing. While the Negrito almost all walk very straight, with toes pointing forward or slightly inward, and very low arches are common, it was equally common among the Bagabos to see high arches more or less in association with ectroversion.

Figure 23.-Standing posture of Bontoc Igorote. Posture during walking.
Their legs are straight; I don't think they have anything to do with O-legs.
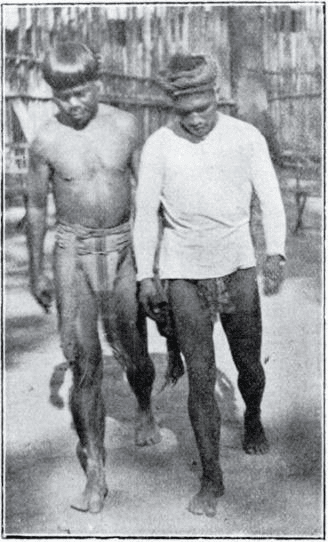
Figure 24.-Gait of Igorotes of the Bontoc and Suyoc tribes. Posture during walking.
YOSHIRO WALKING is this way of walking. If you are used to wearing shoes, you can't do it well.
I must confess that I was a bit disappointed to find that upright or leverage walking was not as common among primitive peoples as I had thought. On the whole, however, it is much more common than among the shoe-wearing peoples. As noted above, upright or lever-walking was almost universal among the Negrito (Figures 21 and 22), and it was more common among the Bontocquigorotes (Figures 23 and 24). It was less common among the Suyoc Igorotes and even less common among the Moro. In contrast, a very pronounced external gait was predominant among the Bagobo (Figure 25)

Figure 25.-Bagobo tribe walking and a group of Bagobo standing in the background.
In most cases, the position of the feet when standing matched the position of the feet when walking slowly. When walking fast, the toes pointed more inward than those who abducted when walking slowly.
In the Central African group, 8 individuals were examined. That is, 4 pygmies, 2 bakuba, 1 chili-chili, and 1 barba. All had fine arches on their feet except for Barba. Barba had few arches in his feet, but his feet were strong and symptom free. Barba had 20 degrees of eversion, i.e., each foot was 10 degrees off the midline. One of the pygmies had the same degree of eversion, and the arch of his foot was very good. Three of the group walked very straight, one had 3 degrees, one had 16 degrees, and one had 18 degrees of eversion. The degree of eversion is the angle between the inner edges of the feet. Of course, the eversion of each foot was only half of the record.
The structure of the feet did not reveal any cause for the differences in the way they walked. It is possible that lifestyle and local land conditions had something to do with it, but I must confess that my investigations in this direction were not very enthusiastic.
Finally.
The relative length of the foot and its component parts is virtually the same whether the foot is laced barefoot or laced with shoes. Until the shoes are worn, the shape, function, and range of voluntary and passive movement of the foot are the same in both, after which the characteristic deformities develop and function is inhibited. In this case, as in the others, the acquired features are not transmitted. The child of a shoe wearer inherits the same foot type as the child of a barefooted race, and this type changes only insofar as the footwear alters it.
The height and shape of the longitudinal arches have nothing to do with the strength or usefulness of the foot. Fragility of the arch is rarely accompanied by fracture or descent, and flatfoot as a pathological entity is almost non-existent.
These studies, while pleasant tasks that took up the ordinary hours of my daily life, were not as thorough as I would have liked. These studies were made possible by the assistance of Dr. W.J. McGee, Dean of the Anthropology Department of the Louisiana Purchase Exposition, and Dr. W.P. Wilson, Chairman of the Philippine Exposition Committee.
It was presented at the Society's 19th Annual Meeting held in Boston on July 6, 7, and 8, 1905.
discussion
Dr. Henry Lynn Taylor of New York wishes to express his deep interest and appreciation for this study and the interesting results obtained. Such information should be more widely disseminated so that it is widely known to the general public. The relationship between the shape of the foot and the wearing of shoes, the posture of standing and walking, etc., if understood and applied by professionals in various fields, especially those involved in gymnastics, military training, and store and factory work, will improve efficiency and reduce suffering.
Dr. AH Freiberg wanted to know how long after the shoes were removed from the feet the tracing took place. He thought that tracings made immediately after the shoes were removed would show more compression than tracings made some time later. He also asked about what is considered Negro in a study of Negro feet. He stated that there are quite a few shades of black in Cincinnati and very few actual blacks. Unless otherwise specified, the survey used only the latter. He felt it was important to know how much white blood was mixed with black blood for the results.
Dr. Halstead Myers of New York, in regard to the statement that the height of the sole and the overall shape of the foot are not a measure of symptoms, said that he believes the same is true for Caucasians and that one cannot always determine what the symptoms are from the shape of the foot.
Dr. John Ridlon stated that it is not always the case to diagnose flat feet or early symptoms of flat feet just because a steel support relieves pain. The steel support may relieve foot pain, or the pain may not be due to flat feet but to a lack of normal dorsiflexion due to shortening of the calf muscles, or what Schaffer called non-deforming medial foot.
Dr. Phil Hoffman concluded by stating that all of the cases included in the primitive analysis were barefoot except for five Ainu who wore sandals. Later for comparison he collected 200 whites and 100 blacks wearing shoes. In examining the latter, he endeavored to secure as many persons of pure African blood as possible. Among the exhibit shoe wearers, almost all cases showed some degree of hallux valgus, but no special attention was paid to the relationship between the two. The symptomatic group was selected from the Caucasian population for the purpose of comparison with the symptomless Caucasian feet. Not a single symptomatic primitive foot was found. All had strong feet. The diagnosis of weak arches was based on a symptom complex and not on the fact that arch support reduced pain.